MELD 3.0 Explained
MELD 3.0 Explained: How the Liver Transplant Scoring System Works
MELD 3.0 is a laboratory-based scoring formula, implemented by the US Organ Procurement and Transplantation Network (OPTN) on 13 July 2023, that predicts 90-day mortality risk for adults with chronic liver disease. It calculates a score from six inputs — bilirubin, creatinine, INR, sodium, albumin and sex — to prioritise patients on the liver transplant waiting list. It replaced MELD-Na largely to address reduced access to liver transplantation and increased risk of mortality or delisting among women under earlier scoring formulas.
Introduction
If you or someone you love is being assessed for a liver transplant in the United States, you will almost certainly hear the term MELD 3.0. It is the formula clinicians use to rank patients on the transplant waiting list by how urgently they need a new liver. Understanding what goes into the score — and what changed from earlier versions — can make consultations with a hepatology team far less confusing. This article explains what MELD 3.0 measures, how it is calculated, why it replaced MELD-Na, and its known strengths and limitations, based on peer-reviewed research and official OPTN documentation.
Key Takeaways
- Standard for US adult liver allocation since 13 July 2023, adding albumin and sex to bilirubin, creatinine, INR and sodium.
- Designed to narrow the long-standing sex gap in transplant access.
- Score range: 6–40; higher means more urgent need — a prognostic tool, not a diagnostic one.
- Other countries use their own adapted models (e.g. GEMA-Na, reMELD-Na) rather than MELD 3.0 directly.
1. What Is MELD 3.0?
MELD 3.0 (Model for End-Stage Liver Disease, version 3.0) is a composite score used to predict mortality due to liver disease. It is the tool used by transplant centres across the United States to decide, among candidates on the waiting list, who receives priority when a donor liver becomes available.
The MELD family originated from work on a method for using laboratory values to evaluate the severity of a patient's chronic liver disease, specifically regarding three-month survival, to assess candidacy for transjugular intrahepatic portosystemic shunt (TIPS) placement. Its predictive strength for short-term mortality led to broader adoption, and the OPTN adopted MELD for national liver transplant allocation in 2002.
MELD 3.0 is the third major iteration. Offers under it remain continuous rather than banded: the MELD score is a continuous scale with no fixed categories — organs go to the patient with the highest MELD in the compatible donor pool.
2. A Brief History: From MELD to MELD 3.0
| Version | Introduced | Key variables | Main change |
|---|---|---|---|
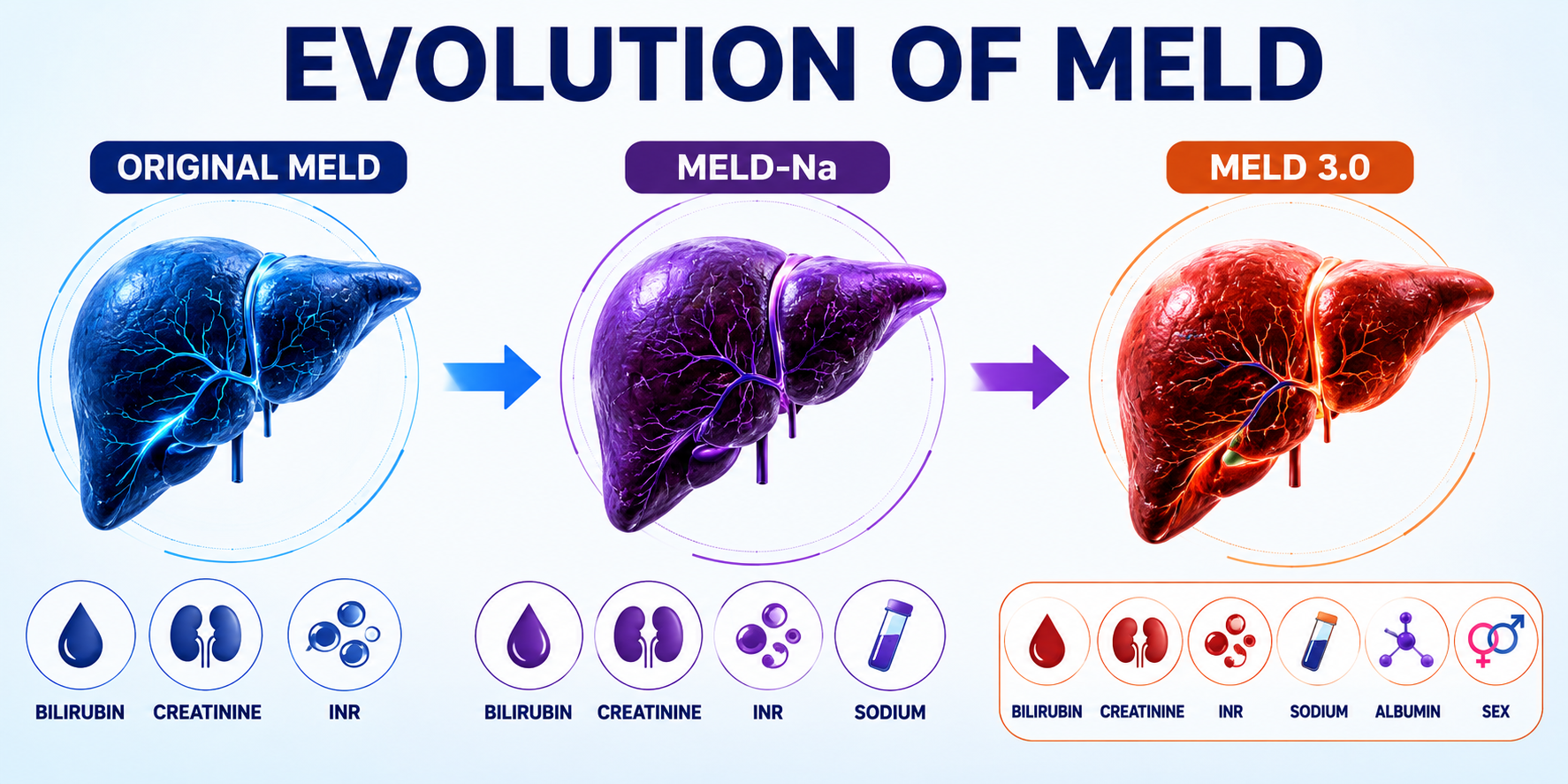
| Original MELD | 2002 (national allocation) | Bilirubin, creatinine, INR | First laboratory-based, objective allocation score |
| MELD-Na | 2016 | Adds sodium | Corrected for hyponatraemia-related mortality risk |
| MELD 3.0 | July 2023 | Adds albumin and sex; revises coefficients | Improves accuracy and reduces sex-based disparity |
Originally, MELD relied solely on serum creatinine, total bilirubin, and INR. MELD-Na followed in 2016, incorporating sodium because lower sodium levels indicate a poorer prognosis. Development of the next iteration followed soon after: MELD 3.0 was proposed to improve upon MELD-Na by adding sex and albumin, and by resetting the upper bound of serum creatinine to 3.0 mg/dL from 4.0 mg/dL. The OPTN Board approved the policy in mid-2022, and implementation followed in two phases: Phase 1 on 15 June 2023 allowed programmes to enter required data, while Phase 2 — when MELD 3.0 began determining allocation — followed on 13 July 2023.
3. How the MELD 3.0 Score Is Calculated
MELD 3.0 combines six clinical inputs into a single numerical score.
Inputs used in MELD 3.0:
- Serum bilirubin (mg/dL)
- Serum creatinine (mg/dL)
- International Normalised Ratio (INR)
- Serum sodium (mmol/L)
- Serum albumin (g/dL)
- Sex (male or female)
According to the model developers, MELD 3.0 improves prediction accuracy by updating the coefficients for each variable, adding albumin as a factor, introducing interaction terms between variables, and lowering the maximum creatinine value used from 4.0 to 3.0 mg/dL. Boundary adjustments apply to several inputs too, following long-standing MELD conventions where creatinine, bilirubin and INR values below 1.0 are set to 1.0, with a further cap applied for patients on dialysis.
The output is a whole-number score, and the maximum MELD score under current OPTN policy is capped at 40. In practice, few clinicians or patients work through the formula by hand — official calculators are provided by OPTN/UNOS and validated tools such as MDCalc, with hospitals entering raw lab values directly.
Practical note: Because MELD 3.0 depends on live lab results, clinicians should periodically re-assess the score, as it changes with changing lab values, and re-certification frequency increases as scores rise.
4. MELD-Na vs MELD 3.0: What Actually Changed
| Feature | MELD-Na | MELD 3.0 |
|---|---|---|
| Core labs | Bilirubin, creatinine, INR, sodium | Same four, plus albumin |
| Sex included | No | Yes |
| Creatinine ceiling | 4.0 mg/dL | 3.0 mg/dL |
| Coefficients | 2016 model | Re-estimated on more recent OPTN data |
| Interaction terms | None | Included between variables |
| Primary goal | Correct for hyponatraemia risk | Improve accuracy and reduce sex disparity |
The shift is not cosmetic: analysis of the OPTN registry treats these as genuinely distinct "MELD eras" for research purposes — MELD 1.0 (2002–2016), MELD 2.0/MELD-Na (2016–2022), and MELD 3.0 (2022–present).
5. Why Sex and Albumin Were Added
This is the single most important change for many readers, because it addresses a documented equity problem. Before MELD 3.0, research consistently found women disadvantaged in transplant access relative to men with similar disease severity. A large nationwide cohort study found that women had reduced access to liver transplant (83.7% vs 85.9%) and an increased risk of mortality or delisting for sickness at 90 days, with female sex remaining an independent risk factor under MELD or MELD-Na but losing its statistical significance under GEMA-Na or MELD 3.0.
The disparity is partly biological and partly measurement-related: creatinine, used in every MELD version to track kidney function, tends to under-represent reduced kidney function in people with lower muscle mass — disproportionately affecting women. Adding albumin and a direct sex adjustment helped correct for this.
Early data are encouraging. One analysis of the year following implementation found that MELD 3.0 had the intended effect of decreasing the sex disparity in probabilities for transplantation and waitlist death, with data from the latter six months suggesting the disparity may be lessening further over time. A separate study similarly found that the July 2023 implementation was associated with women experiencing greater relative increases in top-five organ offer rates than men, both immediately and at three months post-implementation.
6. How MELD 3.0 Scores Are Used in Practice
MELD 3.0 does not determine transplant eligibility on its own — it determines priority among candidates already listed. General clinical guidance suggests considering referral to a hepatologist or liver transplant centre for patients with a MELD score of 10 or higher, though this threshold predates MELD 3.0 and centre practice varies.
Because the score is dynamic, higher-scoring candidates are monitored more closely, with lab values resubmitted on a schedule that shortens as the score rises.
Patients with hepatocellular carcinoma (HCC) may also receive standardised "exception points" rather than relying solely on their calculated score, because many patients with early HCC have well-compensated cirrhosis and low MELD scores of 6–12, yet face significant mortality risk from tumour progression if transplantation is delayed. Exception points follow defined OPTN criteria, including the Milan criteria for tumour size and spread.
7. Benefits of MELD 3.0
- Improved fairness by sex. Early outcome data show a narrowing gap in transplant access and waitlist mortality between men and women.
- Better statistical fit. The model was built by considering both biomedical insight and statistical significance when selecting parameters, incorporating objective, generalisable and easily verifiable variables.
- Retains simplicity. Despite the added variables, it still relies on routine blood tests available at any transplant-capable hospital.
- Transparent, continuous ranking. Allocation uses a continuous score rather than broad categories, reducing arbitrary cut-off effects.
8. Limitations and Criticisms
- HCC remains a structural limitation. HCC represents the most important limitation of the MELD score, since tumour risk doesn't always track liver synthetic function.
- Performance may plateau at higher scores. A bariatric-surgery cohort study found predicted mortality stayed below 1% at a MELD 3.0 of 13 and below 4% at 18, but predictiveness decreased above roughly 19, due to limited data at the extremes.
- International comparisons show mixed results. In Spain, GEMA-Na achieved a higher discrimination statistic (Hc = 0.753) than MELD 3.0 (Hc = 0.726) for non-tumour candidates, though both showed adequate calibration.
- Not validated for every clinical use. Its utility for risk stratification in cirrhotic patients undergoing major abdominal surgery or TIPS placement requires further study.
- Symptom burden isn't fully captured. Complications like ascites and hepatic encephalopathy carry prognostic weight of their own, which is why research into this continues.
9. MELD 3.0 Around the World
MELD 3.0 is a US-specific policy tool, developed and implemented through the OPTN. Other transplant systems have adapted rather than adopted it wholesale: Germany introduced reMELD-Na in March 2025, while Spain developed GEMA-Na, which some analyses found to outperform MELD 3.0 in non-tumour candidates, as noted above. If you're researching liver transplant scoring outside the US, confirm which model your local network uses, since terminology and thresholds aren't interchangeable across systems.
10. Common Mistakes and Misunderstandings
- Treating it as a diagnosis. It's a prognostic and allocation tool, not a diagnostic test for the underlying disease.
- Assuming a single lab draw is final. Scores are reassessed regularly and can change quickly.
- Confusing it with Child-Pugh. Child-Pugh includes clinical signs like ascites and encephalopathy directly; MELD 3.0 is laboratory-based.
- Assuming a "low" score means low risk. It doesn't rule out complications like variceal bleeding, particularly with HCC.
- Believing MELD 3.0 is used globally. Several countries use their own adapted formulas instead.
11. Frequently Asked Questions
What is a good MELD 3.0 score?
There's no single "good" score — lower scores generally mean lower short-term mortality risk, but the score ranks candidates relatively against each other rather than acting as a pass/fail threshold.
What is the highest MELD 3.0 score?
The maximum under current OPTN policy is 40.
Does MELD 3.0 apply to children?
No. Paediatric candidates use PELD or PELD-Cr instead.
Why was albumin added to MELD 3.0?
Albumin reflects liver synthetic function and nutritional status; its inclusion, alongside sex, improved predictive accuracy and helped correct earlier sex-based disparities.
Is MELD 3.0 used outside the United States?
Not directly as policy — several countries have their own adapted versions, such as GEMA-Na in Spain and reMELD-Na in Germany.
How is MELD 3.0 different from MELD-Na?
It adds serum albumin and sex, lowers the creatinine ceiling, updates the statistical coefficients, and adds interaction terms between variables.
When did MELD 3.0 become the US standard?
Full implementation occurred on 13 July 2023, after a preparatory data-entry phase beginning 15 June 2023.
Can I calculate my own MELD 3.0 score at home?
Validated calculators exist, but scores should be interpreted by your transplant team, since exception points and comorbidities materially affect real-world prioritisation.
Does MELD 3.0 replace clinical judgement?
No — it's one input among several, including exception-point systems for conditions like HCC.
Is MELD 3.0 the final version of this scoring system?
Unlikely. Given the pattern of prior revisions and ongoing research into refinements, further iterations are plausible as more outcome data accumulate.
Conclusion
MELD 3.0 is a meaningful, evidence-driven refinement of how the United States prioritises patients for liver transplantation. By adding albumin and sex to the established bilirubin, creatinine, INR and sodium measures, it was built to correct a documented disparity that left women with lower transplant access and higher waitlist mortality than men with comparable disease severity. Early post-implementation data suggest this goal is being met, though the score — like every version before it — has acknowledged limits, particularly around hepatocellular carcinoma and very high-score patients.
If you are navigating a liver transplant assessment, use this article as a starting point for informed conversations with your transplant team, not as a substitute for their guidance.
Looking for a Smarter Way to Track Liver Health?
Try it stress-free — We never modify medical data without your confirmation.